


 Sign Out
Sign Out




The most common adverse reactions with Oncaspar (observed in at least 2 studies with a frequency of >10%) included: alanine aminotransferase increased, aspartate aminotransferase increased, blood bilirubin increased, activated partial thromboplastin time prolonged, hypertriglyceridaemia, hyperglycaemia, and febrile neutropenia.
The most common, severe adverse reactions with Oncaspar (graded 3 or 4) observed in studies DFCI 11-001 and AALL07P4 with a frequency of >5% included: alanine aminotransferase increased, aspartate aminotransferase increased, blood bilirubin increased, febrile neutropenia, hyperglycaemia, lipase increased, and pancreatitis.
Tabulated list of adverse reactions: Adverse reactions and their frequencies are reported in Table 3. Frequencies are defined by the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 3.)
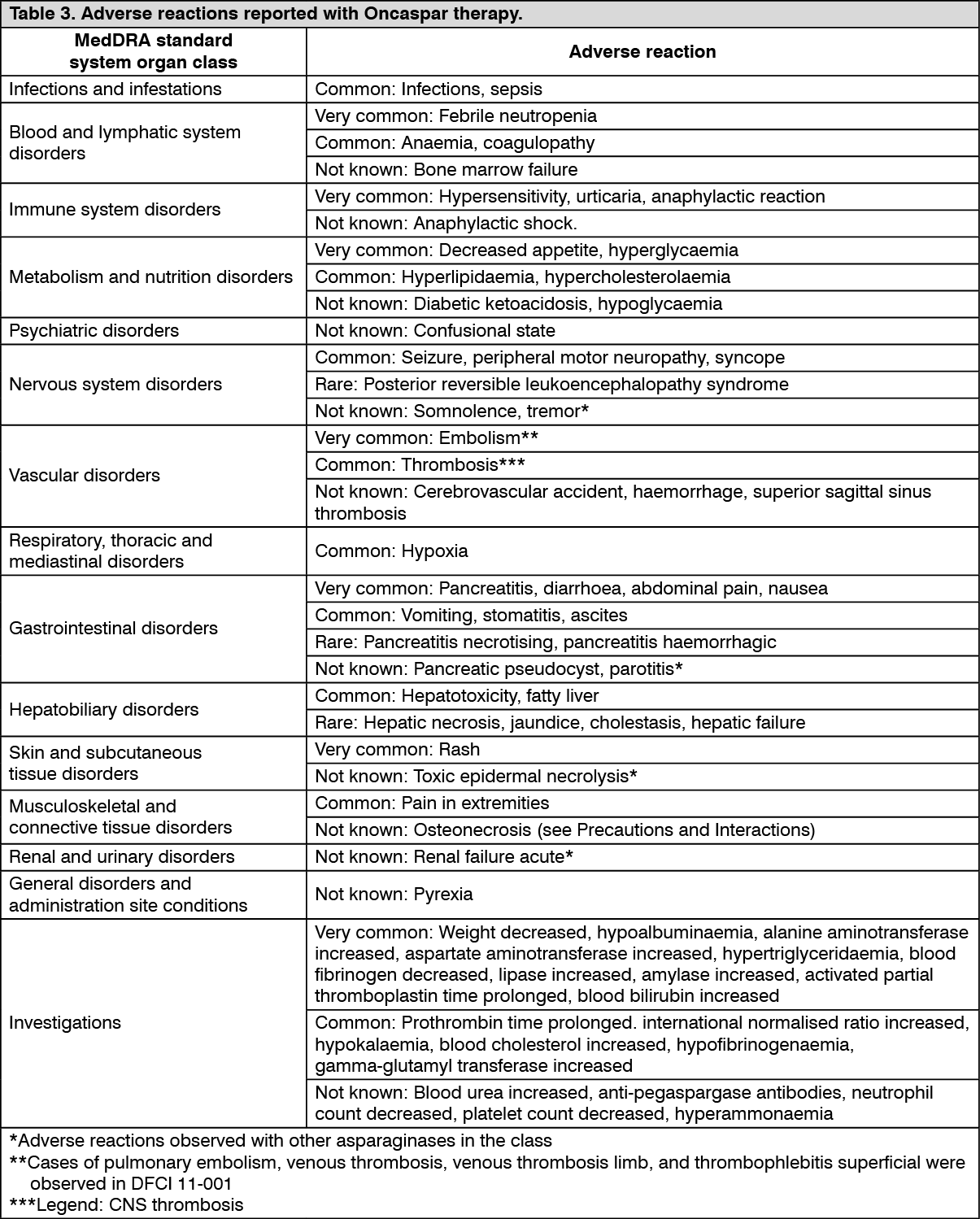 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: The following adverse reactions have been observed in association with asparaginase therapy. Although they have not been specifically associated with the use or pegaspargase, they may occur with the use of Oncaspar.
Blood and lymphatic system disorders: Oncaspar can cause mild to moderate myelosuppression, and all three blood cell lines can be affected. About half of all serious haemorrhages and thromboses affect cerebral vessels and can lead to e.g., stroke, seizure, headache or loss of consciousness.
Nervous system disorders: Oncaspar may cause central nervous system dysfunctions manifesting as convulsions, and less frequently confusional state and somnolence (mildly impaired consciousness).
In rare cases, a reversible posterior leukoencephalopathy syndrome (RPLS) may occur. In very rare cases, mild tremor in the fingers has been described.
Gastrointestinal disorders: About half of patients develop mild to moderate gastrointestinal reactions such as loss of appetite, nausea, vomiting, abdominal cramps, diarrhoea and weight loss.
Acute pancreatitis can occur commonly. There have been isolated reports of formation of pseudocysts (up to four months after the last treatment).
Haemorrhagic or necrotising pancreatitis occurs rarely. One case of pancreatitis with simultaneous acute parotitis has been described with L-asparaginase treatment. In single cases, haemorrhagic or necrotising pancreatitis with fatal outcome has been reported.
Serum amylase can rise during and also after the conclusion of Oncaspar therapy.
Renal and urinary disorders: Acute renal failure may develop in rare cases during treatment with L-asparaginase-containing regimens.
Skin and subcutaneous tissue disorders: Allergic reactions can manifest on the skin. One case of toxic epidermal necrolysis (Lyell's syndrome) has been described in association with L-asparaginase.
Endocrine disorders: Alterations in endocrine pancreatic function are observed commonly and are expressed mainly in the form of abnormal glucose metabolism. Both diabetic ketoacidosis and hyperosmolar hyperglycaemia have been described, which generally respond to administration of insulin.
Metabolism and nutrition disorders: An alteration in serum lipid levels was observed and changes in serum lipid values, in most cases without clinical symptoms, are very common.
A rise in serum urea occurs regularly, is dose-independent and nearly always a sign of pre-renal metabolic imbalance.
General disorders and administration site conditions: Pyrexia can occur after the injection, which usually subsides spontaneously.
Immune system disorders: Specific antibodies to pegaspargase have been detected; uncommonly they were associated with hypersensitivity reactions. Neutralising antibodies reducing clinical efficacy were also recorded.
Hypersensitivity reactions to Oncaspar, including life-threatening anaphylaxis, angioedema, lip swelling, eye swelling, erythema, blood pressure decreased, bronchospasm, dyspnoea, pruritus and rash, can occur during therapy (see Contraindications and Precautions).
Hepatobiliary disorders: Alteration of liver parameters is common. A dose-independent rise in serum transaminases, and serum bilirubin is commonly observed.
Fatty liver can be observed very frequently. There have been rare reports of cholestasis, icterus, hepatic cell necrosis and hepatic failure with fatal outcome.
Impaired protein synthesis can lead to a decline in the serum proteins. There is a dose-independent decrease in serum albumin in the majority of patients during the treatment.
The types of adverse reactions with Oncaspar are similar to those observed with native non-pegylated L-asparaginase (e.g., native E. coli asparaginase).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
View ADR Monitoring Form