Adult: Assisted ventilation (undergoing procedures of at least 45 min): Initially, 130-245 mcg/kg, followed by maintenance doses of 0.5-1.5 mcg/kg per minute or by an inhalation anaesth. Assisted ventilation (intensive care): Initially, a loading dose of 5 mg in divided doses over 10 min (slower if hypotension/bradycardia occur); or via infusion at a rate of 2 mg/hr. Therapy should not exceed 4 days. Elderly: Dose or frequency reduction may be necessary. Child: ≥12 yr Initially, 10-20 mcg/kg as bolus, w/ supplements of 5-10 mcg/kg.
Intravenous Analgesia in patients with spontaneous respiration
Adult: Patient receiving monitored anaesthesia care (MAC): Initially, 3-8 mcg/kg, followed by supplements of 3-5 mcg/kg every 5-20 min; or an infusion of 0.25-1 mcg/kg per min. Elderly: Dose or frequency reduction may be necessary. Child: ≥12 yr Same as adult dose.
Intravenous Adjunct in maintenance of general anaesthesia
Adult: Spontaneous respiration: Initially, up to 500 mcg given slowly over 30 seconds w/ supplements of 250 mcg. Assisted ventilation: Initially, 30-50 mcg/kg w/ supplements of 15 mcg/kg; alternatively, an initial loading dose of 50-100 mcg/kg as a bolus or via infusion over 10 min, followed by infusion at 0.5-1 mcg/kg per min. Maintenance infusion should be stopped 10-30 min the anticipated end of surgery. Elderly: Dose or frequency reduction may be necessary. Child: Maintenance: 0.5-2 mcg/kg per min infusion rate (1 mcg/kg per min when given with IV anaesth), titrated according to response.
Special Patient Group
Debilitated patient: Dose or frequency reduction may be necessary.
Reconstitution
Dilute w/ IV NaCl 0.9%, dextrose 5% in water, or compound Na lactate (Hartmann’s soln) infusions, and use w/in 24 hr of preparation.
Incompatibility
Y-site admin: Incompatible w/ ampothericin B cholesteryl sulfate complex, thiopental.
Contraindications
Obstructive airway disease, resp depression. Admin in labour or before clamping of cord during caesarean section. Concomitant use during or w/in 14 days of MAOI therapy.
Special Precautions
Patient w/ hypovolaemia, CV disease (e.g. acute MI), bradyarrhythmias, history of drug abuse or acute alcoholism, head injury, intracranial lesions, increased intracranial pressure, pulmonary disease, decreased resp reserve, compromised respiration, COPD or other obstructive pulmonary disease, kyphoscoliosis or other skeletal disorder, and compromised intracerebral compliance, hypothyroidism. Hepatic and renal impairment. Elderly and debilitated patients. Childn. Pregnancy and lactation.
This drug may cause impaired cognitive function, if affected, do not drive or operate machinery.
Monitoring Parameters
Continuously monitor vital signs, oxygen saturation, BP, and heart rate. Monitor the patient well after surgery for delayed effects.
Overdosage
Symptoms: Bradycardia, hypoventilation/apnoea, muscle rigidity, hypovolaemia, resp depression. Management: Treat bradycardia w/ anticholinergics (e.g. atropine, glycopyrrolate). Treat hypoventilation/apnoea w/ admin of oxygen, and establishment of patient airway and assisted/controlled ventilation. Treat muscle rigidity w/ IV neuromuscular blocker. Treat resp depression w/ an opioid antagonist (e.g. naloxone). IV fluids and vasoactive agents may be beneficial to manage haemodynamic instability.
Drug Interactions
Increased risk of prolonged/delayed resp depression w/ CYP3A4 isoenzyme inhibitors (e.g. ketoconazole, itraconazole, fluconazole, voriconazole, ritonavir, erythromycin, diltiazem, cimetidine). Enhanced resp depressant effect w/ barbiturates, benzodiazepines, neuroleptics, halogenic gases, and non-selective CNS depressants (e.g. alcohol). May increase blood concentration of propofol by 17%. May predispose to bradycardia or hypotension w/ drugs that depress the heart or increase vagal tone (e.g. β-blockers, anaesth agents). May cause bradycardia and cardiac arrest w/ non-vagolytic muscle relaxants.
Potentially Fatal: Rarely, may cause severe and unpredictable potentiation of MAOIs.
Action
Description: Mechanism of Action: Alfentanil is a short-acting opioid analgesic related to fentanyl. It binds w/ stereospecific receptors w/in the CNS, thereby altering pain perception, increasing pain threshold, and inhibiting ascending pain pathways. Onset: W/in 5 min. Duration: 30-60 min (dose-dependent). Pharmacokinetics: Distribution: Crosses the placenta and blood-brain barrier. Detected in colostrum. Volume of distribution: 0.4-1 L/kg. Plasma protein binding: 88-92%, mainly to α1-acid glycoprotein. Metabolism: Metabolised in the liver by CYP3A4 enzyme via oxidative N- and O-dealkylation into inactive metabolites. Excretion: Via urine (1% as unchanged). Terminal elimination half-life: 90-111 min.
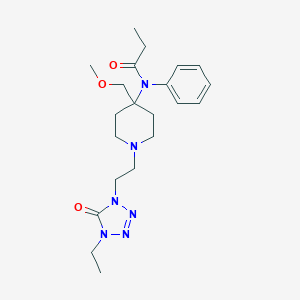
Chemical Structure
Alfentanil Source: National Center for Biotechnology Information. PubChem Database. Alfentanil, CID=51263, https://pubchem.ncbi.nlm.nih.gov/compound/Alfentanil (accessed on Jan. 20, 2020)



 Sign Out
Sign Out