


 Sign Out
Sign Out

Acute psychosis
Adult: 400-800 mg bid. Max: 1.2 g daily. Patients w/ predominantly negative symptoms: 50-300 mg daily.
|
Indications and Dosage
Oral
Acute psychosis Adult: 400-800 mg bid. Max: 1.2 g daily. Patients w/ predominantly negative symptoms: 50-300 mg daily.
|
||||||
|
Renal Impairment
|
||||||
|
Administration
Should be taken on an empty stomach. Preferably taken before meals.
|
||||||
|
Contraindications
Phaeochromocytoma, concomitant prolactin-dependent tumours (e.g. pituitary gland prolactinomas or breast cancer). Pre-pubertal childn. Combination w/ levodopa.
|
||||||
|
Special Precautions
Patient w/ history of epilepsy; Parkinson's disease, CV disease. Avoid abrupt withdrawal. Renal impairment. Elderly. Pregnancy and lactation.
|
||||||
|
Adverse Reactions
Insomnia, anxiety, agitation, drowsiness, wt gain, acute dystonia, parkinsonism, akathisia, tardive dyskinesia, QT prolongation, hypotension, bradycardia, GI disorders (e.g. constipation, nausea, vomiting, dry mouth), hyperglycaemia; breast pain, erectile dysfunction, amenorrhoea, gynaecomastia, galactorrhoea. Rarely, allergic reactions, abnormal LFTs, seizures.
Potentially Fatal: Neuroleptic malignant syndrome. |
||||||
|
Patient Counseling Information
This drug may cause somnolence, if affected, may impair ability to drive or operate machinery.
|
||||||
|
Overdosage
Symptoms: Generalised convulsions, coma, motor restlessness, tachycardia, slight prolongation of the QT interval, drowsiness, sedation, hypotension, extrapyramidal symptoms. Management: Symptomatic and supportive treatment. Institute close supervision of vital functions including continuous cardiac monitoring until patient recovers. Perform gastric lavage. In case severe extrapyramidal symptoms occur, administer anticholinergic agents.
|
||||||
|
Drug Interactions
Increased risk of arrhythmias w/ cisapride, thioridazine, halofantrine, erythromycin, some antiarrhythmics, pimozide, haloperidol, TCAs, β-blockers, some Ca channel blockers, clonidine, guanfacine, digoxin, K-depleting diuretics, lithium, antimalarials. May enhance effects of antihypertensives and CNS depressants (e.g. sedative H1-antihistamines, narcotics, anaesthetics, analgesics, barbiturates, benzodiazepines, other anxiolytics, clonidine and derivatives).
Potentially Fatal: Reciprocal antagonism between levodopa and neuroleptics. |
||||||
|
Food Interaction
May enhance central effects of alcohol.
|
||||||
|
Action
Description:
Mechanism of Action: Amisulpride is a substituted benzamide atypical antipsychotic which binds selectively w/ a high affinity to human dopaminergic D2 and D3 receptor subtypes. Pharmacokinetics: Absorption: Absorbed from GI tract. Bioavailability: Approx 48%. Time to peak plasma concentration: 1 hr (initial); 3-4 hr (2nd). Distribution: Volume of distribution: 5.8 L/kg. Plasma protein binding: Approx 16%. Metabolism: Limited metabolism. Excretion: Mainly via urine as unchanged drug. Terminal elimination half-life: Approx 12 hr. |
||||||
|
Chemical Structure
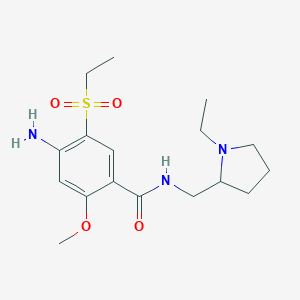 Source: National Center for Biotechnology Information. PubChem Database. Amisulpride, CID=2159, https://pubchem.ncbi.nlm.nih.gov/compound/Amisulpride (accessed on Jan. 20, 2020) |
||||||
|
Storage
Store below 25°C.
|
||||||
|
MIMS Class
|
||||||
|
References
Buckingham R (ed). Amisulpride. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 17/11/2014. Joint Formulary Committee. Amisulpride. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 17/11/2014.
|