Adult: In combination with ≥3 other anti-TB agents when an effective treatment regimen cannot otherwise be provided: Weeks 1-2: 400 mg once daily. Weeks 3-24: 200 mg 3 times a week (with at least 48 hours between doses). Administer by directly observed therapy (DOT). Consider local treatment guidelines when choosing the appropriate combination regimen. Child: 12-<18 years ≥30 kg: Same as adult dose. Treatment recommendations may vary among countries (refer to detailed product or local treatment guidelines).
Administration
tab: Should be taken with food.
Contraindications
Hypersensitivity.
Special Precautions
Patient with heart failure; hypokalaemia, hypocalcaemia, hypomagnesaemia; QTc interval 450-500 milliseconds (derived using Fridericia's formula), personal or family history of congenital QT prolongation; existing or history of hypothyroidism or bradyarrhythmia; history of torsades de pointes. Not intended for use in latent, extrapulmonary (e.g. CNS, bone), or drug-sensitive TB, or infection caused by nontuberculous mycobacteria. Discontinue treatment (including all other QT prolonging drugs) if evidence of QTcF interval is >500 milliseconds (confirmed by repeat ECG) or serious ventricular arrhythmia develops. Moderate to severe hepatic impairment; severe renal impairment (CrCl <30 mL/min) or ESRD requiring haemodialysis or peritoneal dialysis. Children. Pregnancy and lactation. Concomitant use with QT interval prolonging drugs (e.g. ketoconazole, clofazimine).
This drug may cause dizziness, if affected, do not drive or operate machinery.
Monitoring Parameters
Perform culture and susceptibility tests; consult local institutional recommendations before treatment initiation due to risks of antibacterial resistance. Obtain ECG at baseline, after 2 weeks, then monthly during treatment, or more frequently when used concurrently with other QTc interval prolonging drugs or in at-risk patients (e.g. torsades de pointes, congenital long QT syndrome). Monitor serum K, Ca, and Mg (at baseline [correct if necessary] and during treatment); AST, ALT, alkaline phosphatase, and bilirubin (at baseline, monthly during treatment, and as necessary). Monitor for signs and symptoms of hepatic dysfunction. Evaluate sputum specimens every month throughout and at the end of treatment (even if cultures become negative).
Drug Interactions
May reduce exposure and therapeutic effect with moderate or strong CYP3A4 inducers (e.g. rifampicin, efavirenz, carbamazepine, phenytoin); avoid concomitant use. May increase serum concentration with moderate or strong CYP3A4 inhibitors (e.g. ketoconazole, ritonavir, ciprofloxacin, erythromycin); avoid concomitant use for >14 consecutive days unless necessary. Concomitant use with QT interval prolonging drugs including ketoconazole, fluoroquinolones (e.g. moxifloxacin, gatifloxacin), macrolide antibiotics (e.g. clarithromycin), and clofazimine may cause additive or synergistic effects on the QT interval. Hepatotoxic drugs may increase the risk of hepatic-related adverse reactions; avoid concomitant use.
Food Interaction
Administration with food increases bioavailability. Avoid concomitant use with alcohol as it may increase the risk of hepatotoxicity. May reduce exposure and therapeutic effect with St. John's wort; avoid concomitant use.
Action
Description: Mechanism of Action: Bedaquiline is a diarylquinoline antimycobacterial which inhibits the proton transfer chain of mycobacterial ATP synthase, an enzyme necessary for energy generation in Mycobacterium tuberculosis. This action leads to bactericidal effects for both replicating and non-replicating tubercle bacilli. Pharmacokinetics: Absorption: Well absorbed. Increased bioavailability with food. Time to peak plasma concentration: Approx 5 hours. Distribution: Volume of distribution: Approx 164 L. Plasma protein binding: >99.9%. Metabolism: Metabolised in the liver by CYP3A4 isoenzyme to form less potent N-monodesmethyl metabolite (M2). Excretion: Mainly via faeces; urine (≤0.001% as unchanged drug). Terminal elimination half-life: Approx 5.5 months (range: 2-8 months).
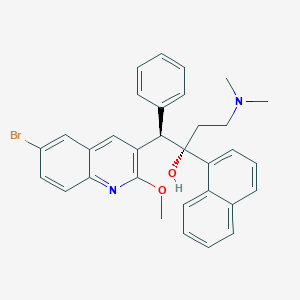
Chemical Structure
Bedaquiline Source: National Center for Biotechnology Information. PubChem Database. Bedaquiline, CID=5388906, https://pubchem.ncbi.nlm.nih.gov/compound/Bedaquiline (accessed on Jan. 21, 2020)
J04AK05 - bedaquiline ; Belongs to the class of other drugs used in the systemic treatment of tuberculosis.
References
Anon. Bedaquiline Fumarate. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 05/10/2021.Anon. Bedaquiline. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 05/10/2021.Buckingham R (ed). Bedaquiline. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 05/10/2021.Janssen-Cilag (New Zealand) Ltd. Sirturo 100 mg Tablets data sheet 31 July 2020. Medsafe. http://www.medsafe.govt.nz. Accessed 05/10/2021.Joint Formulary Committee. Bedaquiline. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 05/10/2021.Sirturo (Janssen-Cilag Ltd.). MIMS Thailand. http://www.mims.com/thailand. Accessed 05/10/2021.Sirturo 100 mg Tablets (Janssen-Cilag Limited). MHRA. https://products.mhra.gov.uk. Accessed 05/10/2021.Sirturo 100 mg Tablets (Johnson & Johnson Sdn Bhd). National Pharmaceutical Regulatory Agency - Ministry of Health Malaysia. https://www.npra.gov.my. Accessed 05/10/2021.Sirturo Tablet (Janssen Products, LP). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 05/10/2021.



 Sign Out
Sign Out