Adult: 1-4 mg once daily or bid. Stop therapy after 1-2 wk to assess whether it is still needed.
Oral Adjunct in parkinsonism
Adult: Arteriosclerotic and idiopathic parkinsonism: Initially, 0.5-1 mg at bedtime, some may initiate 4-6 mg daily. Postencephalitic parkinsonism: Initially, 2 mg daily as a single or in divided doses; may initiate 0.5 mg at bedtime in highly-sensitive patient. Gradually increase dose by 0.5 mg every 5-6 days if necessary. Maintenance: May be given as a single dose at bedtime or in 2-4 divided doses. Max: 6 mg daily.
Parenteral Drug-induced extrapyramidal symptoms
Adult: 1-4 mg once daily or bid by IM or IV inj. Stop therapy after 1-2 wk to assess whether it is still needed.
Parenteral Adjunct in parkinsonism
Adult: Arteriosclerotic and idiopathic parkinsonism: Initially, 0.5-1 mg at bedtime by IM or IV inj, some may initiate 4-6 mg daily. Postencephalitic parkinsonism: Initially, 2 mg daily as a single or in divided doses by IM or IV inj; may initiate 0.5 mg at bedtime in highly-sensitive patient. Gradually increase dose by 0.5 mg every 5-6 days if necessary. Maintenance: May be given as a single dose at bedtime or in 2-4 divided doses. Max: 6 mg daily.
Parenteral Acute dystonia
Adult: 1-2 mg by IM or IV inj. May be followed by 1-2 mg once daily to bid orally for up to 7-28 days to prevent recurrence.
Contraindications
Childn <3 yr.
Special Precautions
Patient w/ tachycardia, obstructive disease of the GI tract (e.g. pyloric or duodenal obstruction), glaucoma, prostatic hyperplasia and/or urinary stricture or retention. Use w/ caution during hot weather (esp in patients concurrently taking atropine-like drugs to chronically ill, alcoholics, w/ CNS disease, those w/ prolonged outdoor exposure). Not intended for treatment of tardive dyskinesia. Pregnancy and lactation.
Adverse Reactions
Tachycardia, dry mouth, constipation, nausea, vomiting, paralytic ileus, toxic psychosis (including exacerbation of pre-existing psychotic symptoms, disorientation, confusion, memory impairment, visual hallucinations, nervousness, depression, listlessness, finger), blurred vision, dilated pupils, dysuria, urinary retention, allergic reactions (e.g. skin rash), fever. Potentially Fatal: Severe anhidrosis which may lead to hyperthermia.
Patient Counseling Information
May impair ability to drive or operate machinery.
Monitoring Parameters
Monitor pulse and anticholinergic effects.
Overdosage
Symptoms: CNS depression preceded or followed by stimulation, nervousness, confusion, listlessness, hallucinations (esp visual), muscle weakness, ataxia, dizziness, dry mouth, mydriasis, blurred vision, glaucoma, palpitations, nausea, vomiting, tachycardia, finger numbness, dysuria, allergic reactions (e.g. skin rash), dysphagia, headache, constipation, convulsions, delirium, shock, resp arrest, anhidrosis, hyperthermia, coma; hot, dry or flushed skin. Management: Symptomatic and supportive treatment. Maintain respiration. Admin short-acting barbiturates for CNS excitement; vasopressor and fluids for circulatory collapse; artificial respiration for severe resp depression; local miotic for mydriasis and cycloplegia; ice bags, other cold applications and alcohol sponges for hyperpyrexia; darken room for photophobia. Admin physostigmine salicylate 1-2 mg via IV/SC inj to reverse symptoms of anticholinergic intoxication. If needed, a 2nd inj may be given after 2 hr.
Drug Interactions
May cause heat intolerance, fever and GI complaints when concomitantly used w/ phenothiazines, haloperidol or other drugs w/ anticholinergic or antidopaminergic activity. May cause paralytic ileus, hyperthermia or heat intolerance (sometimes fatal) when concomitantly used w/ phenothiazines and/or TCAs. Increased sedative effect w/ other CNS depressants (e.g. sedatives and hypnotics, anxiolytics). May interfere w/ oral bioavailability of ketoconazole. Additive depressive effect on GI motility or bladder w/ opiate agonists. Antagonistic effect w/ parasympathomimetics (including both direct cholinergic receptor agonists and cholinesterase inhibitors). Reduced excretion and increased effects w/ carbonic anhydrase inhibitors.
Food Interaction
Increased sedative effect w/ alcohol.
Action
Description: Mechanism of Action: Benzatropine is a centrally-acting anticholinergic agent w/ antihistamine activity. It decreases imbalance between the neurotransmitters acetylcholine and dopamine by antagonising the effect of acetylcholine, thus improving the symptoms of early Parkinson's disease. Onset: W/in a few min (IM/IV); w/in 1 hr (oral). Pharmacokinetics: Absorption: Absorbed from the GI tract. Time to peak plasma concentration: 7 hr (oral). Distribution: Oral: It crosses the blood brain barrier and placenta. Plasma protein binding: Approx 95%. Excretion: Oral: Via faeces (small amount as unchanged drug).
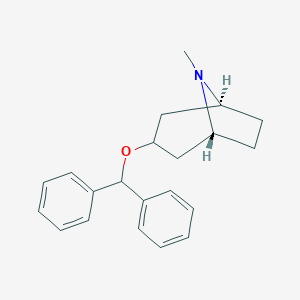
Chemical Structure
Benzatropine Source: National Center for Biotechnology Information. PubChem Database. Benztropine, CID=1201549, https://pubchem.ncbi.nlm.nih.gov/compound/Benztropine (accessed on Jan. 21, 2020)
N04AC01 - benzatropine ; Belongs to the class of anticholinergic agents, ethers of tropine or tropine derivatives. Used in the management of Parkinson's disease.
References
Anon. Benztropine. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 01/12/2015.Benztropine mesylate Injection (Akorn, Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 01/12/2015.Benztropine mesylate Tablet (Bayshore Pharmaceuticals, LLC). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 01/12/2015.Buckingham R (ed). Benzatropine mesilate. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 01/12/2015.McEvoy GK, Snow EK, Miller J et al (eds). Benztropine mesylate. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 01/12/2015.



 Sign Out
Sign Out