Adult: In combination with luteinizing-hormone releasing hormone (LHRH) analogue therapy or surgical castration: 50 mg once daily, to be started at the same time as treatment with LHRH analogue or surgical castration, or alternatively, started at least 3 days before LHRH therapy.
Oral Locally advanced prostate cancer
Adult: As monotherapy or adjuvant therapy to surgery or radiotherapy in patients with high recurrence risk cases: 150 mg once daily, continued for at least 2 years or until disease progression.
Oral Locally advanced, non-metastatic prostate cancer
Adult: In patients whom surgical castration or other medical intervention is inappropriate: 150 mg once daily, continued for at least 2 years or until disease progression.
Administration
May be taken with or without food.
Contraindications
Females. Children. Pregnancy and lactation. Concomitant use of terfenadine, astemizole, or cisapride.
Special Precautions
Patient with history of or risk factors for QT prolongation, heart failure, frequent electrolyte abnormalities; alcohol abuse, family history or risk factors for osteoporosis; diabetes. Moderate to severe hepatic impairment.
Adverse Reactions
Significant: QT prolongation, gynaecomastia, breast pain, anaemia, hepatitis, increased liver enzymes, hypersensitivity reactions (e.g. angioneurotic oedema, urticaria); decreased bone mineral density (prolonged use); loss of glycaemic control and decreased glucose tolerance (in combination with LHRH agonists in diabetic patients). Rarely, photosensitivity reactions. Cardiac disorders: Cardiac failure, chest pain. Gastrointestinal disorders: Abdominal pain, constipation, nausea, dyspepsia, flatulence, diarrhoea. General disorders and administration site conditions: Asthenia. Investigations: Increased weight. Metabolism and nutrition disorders: Decreased appetite, oedema. Nervous system disorders: Dizziness, somnolence. Psychiatric disorders: Depression. Renal and urinary disorders: Haematuria. Reproductive system and breast disorders: Erectile dysfunction, decreased libido. Skin and subcutaneous tissue disorders: Dry skin, alopecia, hirsutism or hair regrowth, pruritus, rash. Vascular disorders: Hot flush. Potentially Fatal: Severe liver injury. Rarely, interstitial lung disease.
Avoid excessive exposure to sunlight or UV light and utilise adequate sun protection (e.g. wear protective clothing, use of sunscreen).
Monitoring Parameters
Monitor LFT at baseline and regularly during the 1st 4 months of therapy, then periodically thereafter; CBC, electrolyte, ECG, echocardiograms, LH, prostate specific antigen, serum testosterone periodically; blood glucose (in diabetic patients), PT and INR (in patients receiving warfarin). Monitor for signs and symptoms of liver dysfunction.
Drug Interactions
Increased risk of haemorrhage with anticoagulants e.g. coumarin. Increased risk of QT interval prolongation or torsade de pointes with class IA (e.g. quinidine, disopyramide) or class III (e.g. amiodarone, sotalol, dofetilide, ibutilide) antiarrhythmic drugs, methadone, moxifloxacin, or antipsychotics. May increase serum levels of ciclosporin and Ca channel blockers. Potentially Fatal: May increase exposure of drugs with narrow therapeutic index such as terfenadine, astemizole, and cisapride.
Action
Description: Mechanism of Action: Bicalutamide is a nonsteroidal antiandrogen. It inhibits the action of androgens by binding to the cytosol androgen receptors in the target tissue without activating gene expression resulting in regression of prostatic tumours. Pharmacokinetics: Absorption: Well absorbed from the gastrointestinal tract. Time to peak plasma concentration: Approx 31 hours ([R]-enantiomer). Distribution: Plasma protein binding: 96%. Metabolism: Undergoes extensive stereospecific metabolism in the liver; the (R)-enantiomer (active) primarily undergoes oxidation to inactive metabolites followed by glucuronidation and the (S)-enantiomer (inactive) primarily undergoes glucuronidation. Excretion: Via urine and faeces. Elimination half-life: Approx 1 week ([R]-enantiomer).
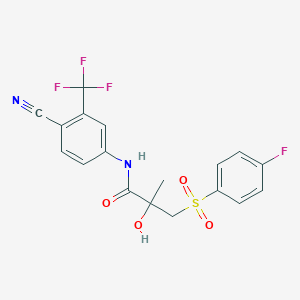
Chemical Structure
Bicalutamide Source: National Center for Biotechnology Information. PubChem Database. Bicalutamide, CID=2375, https://pubchem.ncbi.nlm.nih.gov/compound/Bicalutamide (accessed on Jan. 21, 2020)



 Sign Out
Sign Out