Adult: Initially, 250 mg daily as a single dose in the morning. 5-7 days after treatment initiation, subsequent doses may be increased or decreased by 50-125 mg daily at intervals of 3-5 days until optimum therapeutic control is achieved. Maintenance: 100-500 mg daily. Elderly: Initial: 100-125 mg daily. 5-7 days after treatment initiation, subsequent doses may be increased or decreased by 50-125 mg daily at intervals of 3-5 days until optimum therapeutic control is achieved.
Renal Impairment
Severe: Contraindicated.
Hepatic Impairment
Severe: Contraindicated.
Administration
Should be taken with food.
Contraindications
Type 1 DM, diabetic ketoacidosis (w/ or w/o coma) or other acute complications (e.g. major surgery, severe infection or severe trauma), thyroid impairment. Severe hepatic and renal impairment.
Special Precautions
Hypersensitivity to sulfonamides. Patient w/ condition associated w/ fluid retention, G6PD deficiency. Mild to moderate hepatic and renal impairment. Elderly, debilitated and malnourished patients. Pregnancy and lactation.
Monitor blood glucose, glycosylated Hb level, signs and symptoms of hypoglycaemia.
Overdosage
Symptoms: Hypoglycaemia. Management: Mild hypoglycaemic symptoms w/o loss of consciousness or neurologic findings may be treated w/ oral glucose and adjustments in drug dosage and/or meal patterns. For hypoglycaemic coma, admin rapid IV inj of concentrated (50%) glucose soln followed by continuous infusion of a more dilute (10%) glucose soln.
Drug Interactions
Diminished therapeutic effect w/ thiazide diuretics. Protein-bound drugs (e.g. oral anticoagulants, hydantoins, salicylates, other NSAIDs, sulfonamides) may potentiate hypoglycaemic action of chlorpropamide. Increased plasma concentrations w/ certain antifungals (e.g. miconazole, fluconazole).
Food Interaction
Concurrent alcohol use may cause disulfiram-like reaction.
Action
Description: Mechanism of Action: Chlorpropamide stimulates the secretion of endogenous insulin from β-cells of the pancreas. It also exhibits antidiuretic activity by enhancing vasopressin in the renal tubules. Onset: 1 hr. Duration: 24 hr. Pharmacokinetics: Absorption: Readily absorbed from the GI tract. Time to peak plasma concentration: W/in 2-4 hr. Distribution: It crosses the placenta and enters breast milk. Volume of distribution: 0.13-0.23 L/kg. Plasma protein binding: 90%. Metabolism: Undergoes extensive hepatic metabolism (approx 80%) primarily by CYP2C9 isoenzyme. Excretion: Via urine as metabolites and unchanged drug. Half-life: Approx 35 hr.
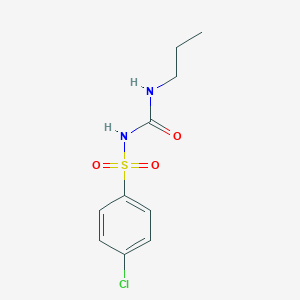
Chemical Structure
Chlorpropamide Source: National Center for Biotechnology Information. PubChem Database. Chlorpropamide, CID=2727, https://pubchem.ncbi.nlm.nih.gov/compound/Chlorpropamide (accessed on Jan. 21, 2020)
Anon. Chlorpropamide. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 15/08/2014.Buckingham R (ed). Chlorpropamide. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 15/08/2014.Chlorpropamide Tablet (Mylan Pharmaceuticals Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 15/08/2014.Diabinese Tablets. U.S. FDA. https://www.fda.gov/. Accessed 15/08/2014.McEvoy GK, Snow EK, Miller J et al (eds). Chlorpropamide. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 15/08/2014.



 Sign Out
Sign Out