Adult: In patients without rest pain or peripheral tissue necrosis; as second-line in patients for whom lifestyle modifications and drug treatment or interventions are insufficient: 100 mg bid. Reassess therapy after 3 months.
Special Patient Group
Patient taking strong or moderate inhibitors of CYP3A4 or CYP2C19 (e.g. certain macrolides, azole antifungals, protease inhibitors, proton pump inhibitors): 50 mg bid.
Renal Impairment
CrCl (mL/min)
Dosage
25
Contraindicated.
Hepatic Impairment
Moderate or severe: Contraindicated.
Administration
Should be taken on an empty stomach. Take at least 30 min before or 2 hr after meals.
Contraindications
Congestive heart failure (of any grade or severity), history of ventricular tachycardia, fibrillation or multifocal ventricular ectopic beats, severe tachyarrhythmia; unstable angina pectoris, myocardial infarction or coronary intervention within the last 6 months; prolonged QTc interval, known predisposition to bleeding (e.g. active peptic ulceration, recent haemorrhagic stroke, proliferative diabetic retinopathy, uncontrolled hypertension) or any active or uncontrolled bleeding. Severe renal (CrCl ≤25 mL/min) and moderate or severe hepatic impairment. Pregnancy and lactation. Concomitant use with ≥2 additional antiplatelet or anticoagulant agents (e.g. aspirin, clopidogrel, heparin, warfarin, dabigatran, rivaroxaban or apixaban).
Special Precautions
Patients with stable coronary disease, atrial or ventricular ectopy, atrial fibrillation or flutter. Surgery including minor invasive measurements (e.g. tooth extraction). Patients taking strong or moderate inhibitors of CYP3A4 or CYP2C19 (e.g. certain macrolides, azole antifungals, protease inhibitors, proton pump inhibitors).
Adverse Reactions
Significant: Tachycardia, palpitation, tachyarrhythmia, hypotension, thrombocytopenia, leucopenia, agranulocytosis. Cardiac disorders: Angina pectoris, ventricular extrasystoles. Gastrointestinal disorders: Diarrhoea, nausea, vomiting, dyspepsia, flatulence, abdominal pain, abnormal faeces. General disorders and admin site conditions: Asthenia. Metabolism and nutrition disorders: Oedema (peripheral, face), anorexia. Nervous system disorders: Headache, dizziness. Respiratory, thoracic and mediastinal disorders: Rhinitis, pharyngitis. Skin and subcutaneous tissue disorders: Ecchymosis, rash, pruritus. Potentially Fatal: Rarely, pancytopenia, aplastic anaemia.
This drug may cause dizziness, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor platelets and WBC count periodically, development of systolic murmur, cardiac symptoms, or signs of bleeding.
Overdosage
Symptoms: Severe headache, diarrhoea, hypotension, tachycardia, cardiac arrhythmias. Management: Supportive treatment. Perform gastric lavage or induce vomiting as necessary to empty stomach contents.
Drug Interactions
Increased serum concentration with strong or moderate inhibitors of CYP3A4 (e.g. erythromycin, ketoconazole, itraconazole, diltiazem) or CYP2C19 (e.g. omeprazole, fluconazole, ticlopidine). Increased serum concentrations of CYP3A4 substrates (e.g. lovastatin, simvastatin, atorvastatin) or other CYP3A4 substrates with narrow therapeutic index (e.g. cisapride, halofantrine, pimozide, ergot alkaloids). Potentially Fatal: Increased risk of bleeding when used concomitantly with antiplatelet or anticoagulant agents (e.g. aspirin, clopidogrel, heparin, warfarin, dabigatran, rivaroxaban or apixaban).
Food Interaction
Increased serum concentration with high-fat meal and grapefruit juice.
Action
Description: Mechanism of Action: Cilostazol inhibits phosphodiesterase-III (PDE-III) resulting to increased cyclic adenosine monophosphate (cAMP) thereby leading to reversible inhibition of platelet aggregation, vasodilation, and inhibition of vascular smooth muscle cell proliferation. Onset: Effect on walking distance: 2-4 weeks; may require up to 12 weeks. Pharmacokinetics: Absorption: Increased absorption if taken with high fat meal. Distribution: Plasma protein binding: 95-98% (cilostazol); 97.4% (3, 4-dehydrocilostazol), 66% (4’-trans-hydroxycilostazol). Metabolism: Extensively metabolised in the liver mainly by CYP3A4, to a lesser extent by CYP2C19, and to an even lesser extent by CYP1A2 and CYP2D6. Excretion: Via urine (74%), faeces (20%) as metabolites. Elimination half-life: Approx 11-13 hours.
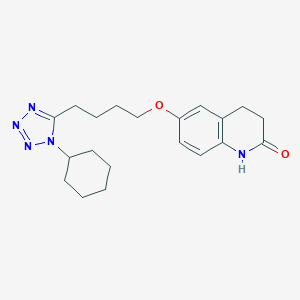
Chemical Structure
Cilostazol Source: National Center for Biotechnology Information. PubChem Database. Cilostazol, CID=2754, https://pubchem.ncbi.nlm.nih.gov/compound/Cilostazol (accessed on Jan. 21, 2020)
B01AC23 - cilostazol ; Belongs to the class of platelet aggregation inhibitors excluding heparin. Used in the treatment of thrombosis.
References
Anon. Cilostazol. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 04/10/2019.Anon. Cilostazol. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 19/09/2019.Buckingham R (ed). Cilostazol. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 19/09/2019.Cilostazol Tablet (Apotex Corp.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 12/02/2016.Cilostazol Tablet (Eon Labs, Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 19/09/2019.Joint Formulary Committee. Cilostazol. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 04/10/2019.



 Sign Out
Sign Out