Adult: 1-3 mg/kg w/in 30 seconds (max: 150 mg), repeated after 5-15 min if required. Child: ≥1 mthSame as adult dose.
Oral Hypoglycaemia
Adult: Initially, 3-5 mg/kg daily in 2 or 3 divided doses. Maintenance: 3-8 mg/kg daily up to 10-15 mg/kg daily in patients w/ refractory hypoglycaemia or insulinoma. Child: Neonates: Initially, 5 mg/kg bid. Maintenance: 1.5-3 mg/kg bid or tid up to 7 mg/kg tid may be required in some cases. ≥1 mth Initially, 1.7 mg/kg tid. Maintenance: 1.5-3 mg/kg bid or tid up to 5 mg/kg tid may be required in some cases.
Renal Impairment
Dose reductions may be necessary.
Incompatibility
Incompatible w/ hydralazine HCl, lidocaine HCl and propranolol HCl.
Contraindications
Management of functional hypoglycaemia.
Special Precautions
Patient in whom retention of Na and water may be hazardous (e.g. impaired cardiac or cerebral circulation); patient w/ aortic coarctation, arteriovenous shunt, heart failure or other cardiac disorders in which increase in cardiac output could be detrimental; hyperuricaemia or history of gout; patient w/ risk factors for pulmonary HTN. Renal impairment. Childn. Pregnancy and lactation.
Adverse Reactions
Inappropriate hypotension and hyperglycaemia, including ketoacidosis and hyperosmolar nonketotic coma; oedema due to salt and water retention, precipitating heart failure; dysgeusia, nausea, anorexia and other GI disturbances, mild hyperuricaemia, extrapyramidal symptoms, eosinophilia and thrombocytopenia, dyspnoea, hypertrichosis, headache, dizziness, tinnitus, blurred vision; hypersensitivity, manifested as rashes, leucopenia and fever. IV: Coronary ischaemia leading to angina, cardiac arrhythmias, marked ECG changes, tachycardia, palpitations, bradycardia; cerebral ischaemia leading to confusion, convulsions, loss of consciousness and neurological deficit; impaired renal function, vasodilatation symptoms, burning sensation in the vein used for inj; pulmonary HTN in neonates and infants.
Monitor BP, glucose levels, white cell and platelet count regularly in prolonged therapy. Regularly assess bone and psychological maturation and growth in childn. Monitor serum uric acid in uremic patients.
Overdosage
Symptoms: Marked hyperglycaemia associated w/ ketoacidosis, severe hypotension. Management: Promptly treat hyperglycaemia w/ insulin and restore fluid and electrolyte balance. If necessary, control hypotension w/ sympathomimetic agents.
Drug Interactions
Enhanced hyperglycaemic, hyperuricemic or hypotensive effects w/ diuretics. Increased risk of hypotension w/ other antihypertensive drugs or vasodilators. Increased risk of hyperglycaemia w/ concomitant phenytoin, corticosteroids or oestrogen-progestogen combinations. May displace other highly protein-bound drugs (e.g. coumarin and its derivatives) resulting in higher blood levels of these substances.
Lab Interference
False-negative insulin response to glucagon.
Action
Description: Mechanism of Action: Diazoxide increases the concentration of glucose in the plasma and inhibits the secretion of insulin by the β-cells of the pancreas, and may increase the hepatic output of glucose. When given IV, it produces a fall in BP by causing vasodilation of the arterioles, thus a reduction in peripheral resistance. It has an antidiuretic action and produces fluid and electrolyte retention. Onset: Hyperglycaemic: W/in 1 hr (oral). Duration: Hyperglycaemic: ≤8 hr (oral). Antihypertensive effect: 3-12 hr (IV). Pharmacokinetics: Absorption: Readily absorbed from the GI tract. Distribution: Crosses the placenta and blood-brain barrier. Plasma protein binding: >90%. Metabolism: Partially metabolised in the liver via oxidation and sulphate conjugation. Excretion: Via urine as unchanged drug (50%) and metabolites; faeces (small amounts). Plasma half-life: Approx 20-45 hr.
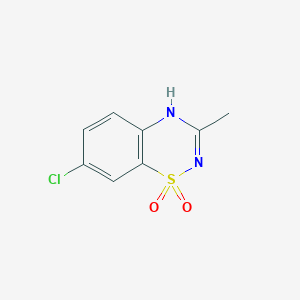
Chemical Structure
Source: National Center for Biotechnology Information. PubChem Database. Diazoxide, CID=3019, https://pubchem.ncbi.nlm.nih.gov/compound/Diazoxide (accessed on Jan. 21, 2020)
Storage
Oral susp: Store between 2-30°C. Protect from light, heat and freezing. Inj soln: Store below 25°C. Protect from light. Avoid excessive heat and freezing.



 Sign Out
Sign Out