Adult: For treatment following 5-10 days of initial therapy with parenteral anticoagulant, and for prophylaxis of recurrent cases: ≤60 kg: 30 mg once daily; >60 kg: 60 mg once daily. Duration of treatment is individualised based on assessment of treatment benefits against the risk for bleeding. Dose modification or discontinuation may be required when switching to and from edoxaban based on patient safety and tolerability (refer to detailed product guidelines).
Oral Prophylaxis of stroke in non-valvular atrial fibrillation, Prophylaxis of systemic embolism in non-valvular atrial fibrillation
Adult: In patients with ≥1 risk factors e.g. CHF, hypertension, age ≥75 years, diabetes mellitus, prior stroke or TIA: ≤60 kg: 30 mg once daily; >60 kg: 60 mg once daily. Dose modification or discontinuation may be required when switching to and from edoxaban based on patient safety and tolerability (refer to detailed product guidelines).
Prophylaxis of stroke and systemic embolism in non-valvular atrial fibrillation:
CrCl (mL/min)
Dosage
<15
Not recommended.
15-50
30 mg once daily.
51-80
60 mg once daily.
>95
Contraindicated.
Deep vein thrombosis; Pulmonary embolism:
CrCl (mL/min)
Dosage
<15
Not recommended.
15-50
30 mg once daily.
51-80
60 mg once daily.
Hepatic Impairment
Moderate to severe: Not recommended.
Administration
film-coated tab: May be taken with or without food.
Contraindications
Active pathological bleeding, lesions, or conditions with significant risk for major bleeding (e.g. current or recent gastrointestinal ulceration, malignant neoplasms at high risk of bleeding, recent brain or spinal injury, recent brain, spinal or ophthalmic surgery, recent intracranial haemorrhage, known or suspected oesophageal varices, arteriovenous malformations, vascular aneurysms or major intraspinal or intracerebral vascular abnormalities), uncontrolled severe hypertension. Hepatic disease associated with coagulopathy and clinically relevant bleeding risk; creatinine clearance of >95 mL/min (when used for prophylaxis of stroke and systemic embolism in non-valvular atrial fibrillation. Pregnancy and lactation. Concomitant use with other anticoagulants (e.g. enoxaparin, dalteparin, heparin derivatives, oral anticoagulants), except under specific circumstances of switching anticoagulant therapy; other drugs that affect haemostasis (e.g. NSAIDs, SSRIs, SNRIs); rifampicin.
Special Precautions
Patient with increased risk of bleeding, ALT/AST >2x ULN or total bilirubin ≥1.5x ULN, body weight ≤60 kg. Patients who are receiving neuraxial anaesthesia or those undergoing spinal, invasive or surgical procedures, or cardioversion. Not recommended for use in patients with moderate to severe mitral stenosis, mechanical heart valves, or during the 1st 3 months after implantation of a bioprosthetic heart valve; history of thrombosis who are diagnosed with triple-positive antiphospholipid syndrome. Not recommended to be used as an alternative to unfractionated heparin in patients with pulmonary embolism who are haemodynamically unstable or may receive thrombolysis or pulmonary embolectomy. If edoxaban is discontinued for a reason other than pathological bleeding or completion of a course of therapy, coverage with another anticoagulant should be considered (refer to detailed product information for the transition guidelines). Renal and hepatic impairment. Patients taking P-gp inhibitors (e.g. ciclosporin, dronedarone, erythromycin, ketoconazole).
Adverse Reactions
Blood and lymphatic system disorders: Anaemia. Gastrointestinal disorders: Abdominal pain, nausea, gastrointestinal or oropharyngeal haemorrhage. General disorders and administration site conditions: Puncture site haemorrhage. Investigations: Increased bilirubin, GGT; abnormal LFT. Nervous system disorders: Dizziness, headache. Renal and urinary disorders: Macroscopic haematuria or urethral haemorrhage. Reproductive system and breast disorders: Vaginal haemorrhage. Respiratory, thoracic and mediastinal disorders: Epistaxis. Skin and subcutaneous tissue disorders: Rash, pruritus, cutaneous soft tissue haemorrhage. Potentially Fatal: Bleeding.
Assess renal and liver functions prior to initiation of treatment and as clinically indicated. Monitor for signs and symptoms of blood loss.
Overdosage
Symptom: Haemorrhage. Management: Individualised according to the severity and location of the haemorrhage. Early administration of activated charcoal may be considered to reduce absorption. Symptomatic treatment could be used as appropriate, e.g. mechanical compression for severe epistaxis, surgical haemostasis with bleeding control procedures, fluid replacement and haemodynamic support, blood products (packed red cells or fresh frozen plasma, depending on associated anaemia or coagulopathy) or platelets. Administer a 4-factor prothrombin
complex concentrate (PCC) at 50 international units/kg for life-threatening bleeding that cannot be controlled by transfusion or haemostasis. Recombinant factor VIIa (r-FVIIa) may also be considered.
Drug Interactions
Increased plasma concentration with P-gp inhibitors (e.g. ciclosporin, dronedarone, erythromycin, ketoconazole, quinidine, verapamil). P-gp inducers, excluding rifampicin (e.g. phenytoin, carbamazepine, phenobarbital) may reduce the plasma concentration of edoxaban. Potentially Fatal: Increased risk of bleeding with other anticoagulants (e.g. enoxaparin, warfarin), antiplatelets (e.g. aspirin), thrombolytics, NSAIDs (e.g. naproxen), SSRIs, SNRIs. Rifampicin significantly reduces the systemic exposure of edoxaban.
Food Interaction
St. John's wort may reduce the plasma concentration of edoxaban.
Lab Interference
Prolongs standard clotting tests (e.g. prothrombin time, INR, aPTT).
Action
Description: Mechanism of Action: Edoxaban is a highly selective, reversible and direct inhibitor of activated factor X (Xa). Factor Xa plays a central role in the blood coagulation cascade by serving as the convergence point for the intrinsic and extrinsic pathways. Inhibition of free factor Xa reduces thrombin generation, prolongs clotting time and decreases the risk of thrombus formation. Pharmacokinetics: Absorption: Absorbed from gastrointestinal tract. Bioavailability: Approx 62%. Time to peak plasma concentration: Within 1-2 hours. Distribution: Volume of distribution: 107 L. Plasma protein binding: Approx 55%. Metabolism: Minimally metabolised via hydrolysis by carboxylesterase 1 to the active metabolite M-4, conjugation, and oxidation by CYP3A4/5 enzyme. Excretion: Via urine (approx 35%, mainly as unchanged drug); remainder via biliary and intestinal excretion. Elimination half-life: 10-14 hours.
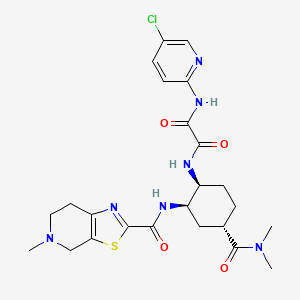
Chemical Structure
Edoxaban Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 10280735, Edoxaban. https://pubchem.ncbi.nlm.nih.gov/compound/Edoxaban. Accessed Nov. 25, 2022.
B01AF03 - edoxaban ; Belongs to the class of direct factor Xa inhibitors. Used in the treatment of thrombosis.
References
Anon. Edoxaban Tosylate. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 24/10/2022.Anon. Edoxaban. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 24/10/2022.Buckingham R (ed). Edoxaban. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 24/10/2022.Joint Formulary Committee. Edoxaban. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 24/10/2022.Lixiana 15 mg, 30 mg and 60 mg Film-coated Tablets (Daiichi Sankyo Europe GmbH). National Pharmaceutical Regulatory Agency - Ministry of Health Malaysia. https://www.npra.gov.my. Accessed 24/10/2022.Lixiana 30 mg Film-coated Tablets (Daiichi Sankyo UK Ltd). MHRA. https://products.mhra.gov.uk. Accessed 24/10/2022.Savaysa Tablet, Film Coated (Daiichi Sankyo Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 24/10/2022.



 Sign Out
Sign Out