Adult: As adjunct in stable patients with LVEF ≤40%: Initially, 25 mg once daily, may increase to 50 mg once daily within 4 weeks, as tolerated. Dose reduction, dosing interruption, or discontinuation may be required according to serum K level (refer to detailed product guideline).
Oral Hypertension
Adult: As monotherapy or in combination with other antihypertensives: Initially, 50 mg once daily, may increase up to Max 50 mg bid, if necessary.
Renal Impairment
Hypertension:
CrCl (mL/min)
Dosage
<50
Contraindicated.
Heart failure post myocardial infarction:
CrCl (mL/min)
Dosage
<30
Contraindicated.
30-60
Initially, 25 mg on alternate days. Adjust dose according to
serum K level.
Administration
May be taken with or without food.
Contraindications
Clinically significant hyperkalaemia (>5.5 mmol/L) at initiation. Severe renal impairment (CrCl <30 mL/min). Concomitant use of strong CYP3A4 inhibitors (e.g. ritonavir, ketoconazole, itraconazole). Patient treated for hypertension: Type 2 diabetes mellitus with microalbuminuria, serum creatinine >2.0 mg/dL (males) or >1.8 mg/dL (females); CrCl <50 mL/min. Concomitant use of K-sparing diuretics (e.g. amiloride, spironolactone, triamterene), K supplements.
Special Precautions
Patient with risk factors for hyperkalaemia (e.g. proteinuria, diabetes mellitus). Moderate renal impairment (CrCl 30-60 mL/min) and moderate to severe hepatic impairment. Elderly. Pregnancy and lactation.
Adverse Reactions
Significant: Hyperkalaemia, urinary tract disorders. Cardiac disorders: Atrial fibrillation, left ventricular failure. Gastrointestinal disorders: Nausea, vomiting, diarrhoea, constipation. General disorders and administration site conditions: Asthenia. Investigations: Increase serum urea, serum creatinine. Musculoskeletal and connective tissue disorders: Muscle spasm, back pain. Nervous system disorders: Headache, dizziness, syncope. Psychiatric disorders: Insomnia. Renal and urinary disorders: Renal impairment. Respiratory, thoracic and mediastinal disorders: Cough. Skin and subcutaneous tissue disorders: Rash, pruritus. Vascular disorders: Hypotension.
Monitor blood pressure and serum K prior to initiation of treatment, within the 1st week, 1 month after dose adjustment or treatment, and periodically thereafter. Heart failure: Monitor serum K and renal function 3 days after initiation of treatment, 1 week after initiation, monthly for the 1st 3 months, and every 3 months thereafter.
Overdosage
Symptoms: Hypotension, hyperkalaemia. Management: Symptomatic and supportive treatment.
Drug Interactions
Increased risk of hyperkalaemia with ACE inhibitors, ARBs. Increased risk of hyperkalaemia and renal impairment with ciclosporin, tacrolimus. Enhanced hypotensive effect with alpha-1 blockers (e.g. alfuzozin, prazosin), TCAs, neuroleptics, amifostine, and baclofen. Decrease antihypertensive effects with NSAIDs, glucocorticoids, and tetracosactide. Potentially Fatal: Significantly increased plasma level with potent CYP3A4 inhibitors (e.g. ketoconazole, ritonavir, itraconazole, nelfinavir, clarithromycin). May enhance hyperkalaemic effect of K-sparing diuretics and K supplements in patients with hypertension.
Food Interaction
Reduced serum concentration with St. John's wort. Increased serum concentration with grapefruit juice.
Lab Interference
May result to false-negative aldosterone/renin ratio.
Action
Description: Mechanism of Action: Eplerenone selectively blocks the binding of aldosterone, a key hormone involved in the regulation of blood pressure and pathophysiology of CV disease, resulting in the inhibition of Na reabsorption in the distal tubule, decreasing water retention, reducing potassium excretion thereby decreasing blood pressure. Pharmacokinetics: Absorption: Absolute bioavailability: 69%. Time to peak plasma concentration: Approx 1.5-2 hours. Distribution: Crosses the placenta. Volume of distribution: 42-90 L. Plasma protein binding: Approx 50%, mainly to α1-acid glycoproteins. Metabolism: Metabolised in the liver by CYP3A4 isoenzymes. Excretion: Via urine (approx 67%); faeces (approx 32%); <5% as unchanged drug in urine and faeces. Elimination half-life: Approx 3-6 hours.
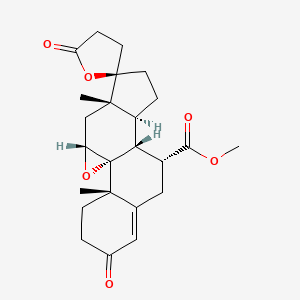
Chemical Structure
Eplerenone Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 443872, Eplerenone. https://pubchem.ncbi.nlm.nih.gov/compound/Eplerenone. Accessed Apr. 27, 2023.
C03DA04 - eplerenone ; Belongs to the class of aldosterone antagonists. Used as potassium-sparing diuretics.
References
Anon. Eplerenone. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 31/03/2023.Anon. Eplerenone. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 31/03/2023.Buckingham R (ed). Eplerenone. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 31/03/2023.Eplerenone 25 mg Film-coated Tablets (Accord Healthcare Limited). MHRA. https://products.mhra.gov.uk. Accessed 31/03/2023.Eplerenone Tablet, Coated (Westminster Pharmaceuticals, LLC). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 31/03/2023.Inspra (Viatris Sdn. Bhd.). National Pharmaceutical Regulatory Agency - Ministry of Health Malaysia. https://www.npra.gov.my. Accessed 31/03/2023.Joint Formulary Committee. Eplerenone. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 31/03/2023.Viatris Ltd. Inspra 25 mg and 50 mg Film-coated Tablets data sheet 02 August 2021. Medsafe. http://www.medsafe.govt.nz. Accessed 31/03/2023.



 Sign Out
Sign Out