Adult: Initially, 560-840 mg daily in divided doses, adjusted to 140-1,400 mg daily according to response and GI tolerance. Assess for possible benefits of continued therapy after 30-90 days. Continue treatment as long as favourable response is maintained.
Hepatic Impairment
Severe: Contraindicated.
Contraindications
Active thrombophlebitis or thromboembolic disorders (except when the actual tumour mass is the cause of phenomenon); peptic ulcer, severe CV disease. Severe hepatic impairment. Pregnancy and lactation. Admin of live vaccines.
Special Precautions
Patient w/ history of thrombophlebitis or thromboembolic disorders esp if associated w/ estrogen therapy, CV/cerebrovascular/coronary artery disease, DM, HTN, epilepsy, migraine, metabolic bone disease associated w/ hypercalcaemia. May exacerbate pre-existing or incipient peripheral oedema or congestive heart disease. Hepatic and renal impairment.
Adverse Reactions
Oestrogenic effects (e.g. gynaecomastia, impotence, fluid retention, CV effects); GI disturbance, nausea, vomiting, hepatic dysfunction, loss of libido, leucopenia, thrombocytopenia. Potentially Fatal: Embolism, MI, CHF, angioedema.
Monitoring Parameters
Monitor BP, LFT, and Ca levels.
Drug Interactions
May increase therapeutic activity and toxicity of TCAs. Decreased absorption w/ drugs containing Ca, Mg or Al (e.g. antacids). Increased risk of angioedema w/ ACE inhibitors. Potentially Fatal: Admin of live vaccines during treatment may result in serious infections due to immunosuppression.
Food Interaction
Milk, milk products and Ca-containing foods may impair absorption.
Lab Interference
May affect endocrine and liver function tests.
Action
Description: Mechanism of Action: Estramustine is a complex of 17-β-estradiol and nitrogen mustard (normustine) linked by a carbamate ester. Estramustine and its oxidised isomer, estromustine, exert their cytotoxic effect by binding to tubulin and/or microtubule-associated proteins, thus inducing depolymerisation of microtubules, resulting in cellular metaphase arrest. Upon hydrolysis, estradiol is released causing a weak antiandrogen effect. Pharmacokinetics: Absorption: Incompletely (approx 75%) absorbed from the GI tract. Reduced absorption w/ food. Bioavailability: 44-75%. Time to peak plasma concentration: 2-4 hr. Distribution: Accumulates in the prostatic carcinoma tissues and plasma. Metabolism: Initially dephosphorylated in the GI tract. Hydrolysed and oxidised in the liver into estromustine, estradiol, and estrone. Excretion: Mainly via faeces; urine (<1% as estradiol and estrone). Plasma half-life: 10-20 hr.
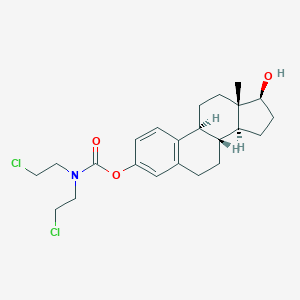
Chemical Structure
Estramustine Source: National Center for Biotechnology Information. PubChem Database. Estramustine, CID=259331, https://pubchem.ncbi.nlm.nih.gov/compound/Estramustine (accessed on Jan. 22, 2020)
L01XX11 - estramustine ; Belongs to the class of other antineoplastic agents. Used in the treatment of cancer.
References
Anon. Estramustine. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 12/07/2016.Buckingham R (ed). Estramustine Sodium Phosphate. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com/. Accessed 12/07/2016.Emcyt Capsule (Pharmacia and Upjohn Company). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 12/07/2016.Joint Formulary Committee. Estramustine Phosphate. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 12/07/2016.McEvoy GK, Snow EK, Miller J et al (eds). Estramustine Phosphate Sodium. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com/mc/ahfs/current/. Accessed 12/07/2016.



 Sign Out
Sign Out