


 Sign Out
Sign Out




Pharmacology: Pharmacodynamics: Mechanism of action: Breztri Aerosphere contains budesonide, a glucocorticosteroid, and two bronchodilators: glycopyrronium, a long-acting muscarinic antagonist (anticholinergic) and formoterol, a long-acting β2-adrenergic agonist.
Budesonide is a glucocorticosteroid which when inhaled has a rapid (within hours) and dose-dependent anti-inflammatory action in the airways.
Glycopyrronium is a long-acting muscarinic antagonist, which is often referred to as an anticholinergic. The major targets for anticholinergic drugs are muscarinic receptors located in the respiratory tract. In the airways, it exhibits pharmacological effects through inhibition of M3 receptor at the smooth muscle leading to bronchodilation. Antagonism is competitive and reversible. Prevention of methylcholine and acetylcholine-induced bronchoconstrictive effects was dose-dependent and lasted more than 12 hours.
Formoterol is a selective β2-adrenergic agonist that when inhaled results in rapid and long-acting relaxation of bronchial smooth muscle in patients with reversible airways obstruction. The bronchodilating effect is dose-dependent, with an onset of effect within 1-3 minutes after inhalation. The duration of effect is at least 12 hours after a single dose.
Clinical efficacy: The efficacy and safety of Breztri Aerosphere was evaluated in patients with moderate to very severe COPD in two randomised, parallel-group trials, ETHOS and KRONOS. Both studies were multicentre, double-blind studies. Patients were symptomatic with a COPD Assessment Test (CAT) score ≥10 while receiving two or more daily maintenance therapies for at least 6 weeks prior to screening.
ETHOS was a 52-week trial (N=8,588 randomised; 60% male, mean age of 65) that compared two inhalations twice daily of Breztri Aerosphere, formoterol fumarate dihydrate/glycopyrronium (FOR/GLY) MDI 5/7.2 micrograms, and formoterol fumarate dihydrate/budesonide (FOR/BUD) MDI 5/160 micrograms. Patients had moderate to very severe COPD (post-bronchodilator FEV1 ≥25% to <65% predicted) and were required to have a history of one or more moderate or severe COPD exacerbations in the year prior to screening. The proportion of patients with moderate, severe and very severe COPD was 29%, 61% and 11% respectively. The mean baseline FEV1 across all groups was 1,021-1,066 mL, and during screening the mean post-bronchodilator percent predicted FEV1 was 43% and mean CAT score was 19.6. The primary endpoint of the ETHOS trial was the rate of on-treatment moderate or severe COPD exacerbations for Breztri Aerosphere compared with FOR/GLY MDI and FOR/BUD MDI.
KRONOS was a 24-week trial (N=1,902 randomised; 71% male, mean age of 65) that compared two inhalations twice daily of Breztri Aerosphere, FOR/GLY MDI 5/7.2 micrograms, FOR/BUD MDI 5/160 micrograms and open-label active comparator formoterol fumarate dihydrate/budesonide Turbuhaler (FOR/BUD TBH) 6/200 micrograms. Patients had moderate to very severe COPD (post-bronchodilator FEV1 ≥25% to <80% predicted). The proportion of patients with moderate, severe and very severe COPD was 49%, 43% and 8% respectively. The mean baseline FEV1 across all groups was 1,050-1,193 mL, and during screening the mean post-bronchodilator percent predicted FEV1 was 50%, over 26% of patients reported a history of one or more moderate or severe COPD exacerbation in the past year and the mean CAT score was 18.3. There was a 28-week extension, for up to 52 weeks of treatment, in a subset of subjects. The primary endpoints of the KRONOS trial were the on-treatment FEV1 area under the curve from 0-4 hours (FEV1 AUC0-4) over 24 weeks for Breztri Aerosphere compared to FOR/BUD MDI and the on-treatment change from baseline in morning pre-dose trough FEV1 over 24 weeks for Breztri Aerosphere compared to FOR/GLY MDI.
At study entry, the most common COPD medications reported in the ETHOS and KRONOS studies were ICS+LABA+LAMA (39%, 27% respectively), ICS+LABA (31%, 38% respectively) and LAMA+LABA (14%, 20% respectively).
Effect on exacerbations: Moderate or severe exacerbations: In the 52-week ETHOS study, Breztri Aerosphere significantly reduced the annual rate of on-treatment moderate/severe exacerbations by 24% (95% CI: 17, 31; p<0.0001) compared with FOR/GLY MDI (rate; 1.08 vs 1.42 events per patient year) and by 13% (95% CI: 5, 21; p=0.0027) compared with FOR/BUD MDI (rate; 1.08 vs 1.24 events per patient year).
The benefits observed on annualised rate of moderate/severe COPD exacerbations over 24 weeks in KRONOS were generally consistent with those observed in ETHOS. Improvements compared with FOR/GLY MDI were statistically significant; however improvements compared with FOR/BUD MDI and FOR/BUD TBH did not reach statistical significance.
Severe exacerbations (resulting in hospitalisation or death): In ETHOS, Breztri Aerosphere numerically reduced the annual rate of on-treatment severe exacerbations by 16% (95% CI: -3, 31; p=0.0944) compared with FOR/GLY MDI (rate; 0.13 vs 0.15 events per patient year) and significantly reduced the annual rate of on-treatment severe exacerbations by 20% (95% CI: 3, 34; p=0.0221) compared with FOR/BUD MDI (rate; 0.13 vs 0.16 events per patient year).
In both studies, benefits on exacerbations were observed in patients with moderate, severe and very severe COPD.
Effects on lung function: In ETHOS and KRONOS, Breztri Aerosphere improved on-treatment lung function (FEV1) compared with FOR/GLY MDI and FOR/BUD MDI (see Table 1 for ETHOS and Table 2 for KRONOS). There was a sustained effect over the 24-week treatment period in both studies, and over 52 weeks in ETHOS. (See Tables 1 and 2.)
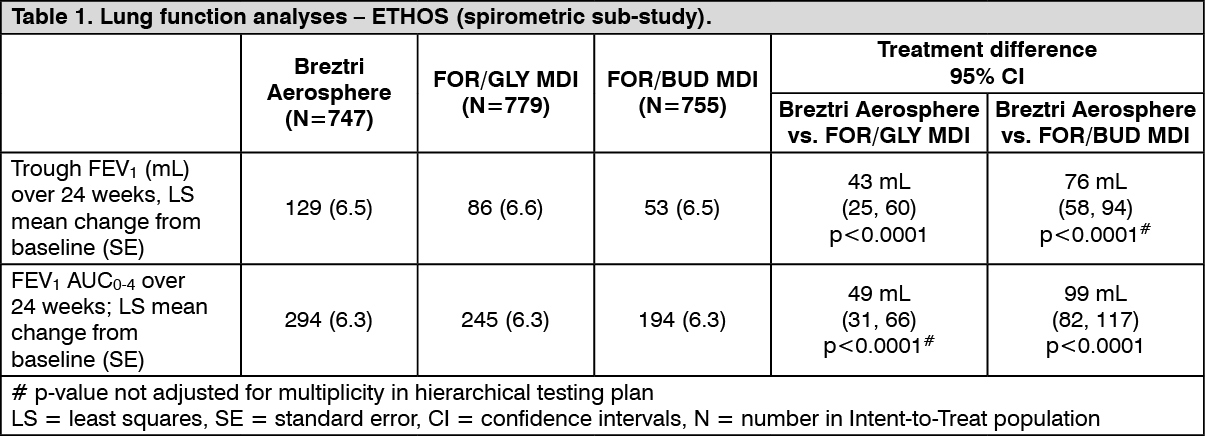 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image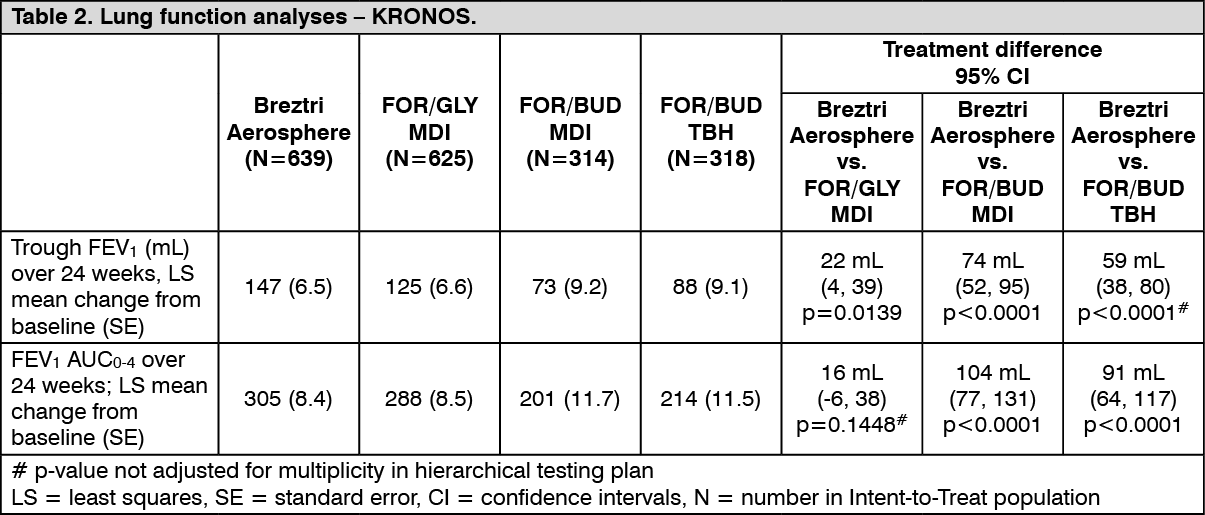 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSymptom relief: In ETHOS, the baseline average dyspnoea scores ranged from 5.8 - 5.9 across the treatment groups. Breztri Aerosphere significantly improved breathlessness (measured using the Transition Dyspnoea Index [TDI] focal score over 24 weeks) compared with FOR/GLY MDI (0.40 units; 95% CI: 0.24, 0.55; p<0.0001) and compared with FOR/BUD MDI (0.31 units; 95% CI: 0.15, 0.46; p<0.0001). Improvements were sustained over 52 weeks. In KRONOS, the baseline average dyspnoea scores ranged from 6.3 - 6.5 across the treatment groups. Breztri Aerosphere significantly improved breathlessness over 24 weeks compared with FOR/BUD TBH (0.46 units; 95% CI: 0.16, 0.77; p=0.0031). Improvements compared with FOR/GLY MDI and FOR/BUD MDI did not reach statistical significance.
Health-related quality of life: In ETHOS, Breztri Aerosphere significantly improved disease-specific health status (as assessed by the St. George's Respiratory Questionnaire [SGRQ] total score) over 24 weeks compared with FOR/GLY MDI (improvement -1.62; 95% CI: -2.27, -0.97; p<0.0001) and compared with FOR/BUD MDI (improvement -1.38; 95% CI: -2.02, -0.73; p<0.0001). Improvements were sustained over 52 weeks. In KRONOS, improvements compared with FOR/GLY MDI, FOR/BUD MDI and FOR/BUD TBH did not reach statistical significance.
Use of rescue medication: In ETHOS, Breztri Aerosphere significantly reduced the on-treatment use of rescue medication over 24 weeks compared with FOR/GLY MDI (treatment difference -0.51 puffs/day; 95% CI: -0.68, -0.34; p<0.0001) and FOR/BUD MDI (treatment difference -0.37 puffs/day; 95% CI: -0.54, -0.20; p<0.0001). Reductions were sustained over 52 weeks. In KRONOS, differences compared with FOR/GLY MDI, FOR/BUD MDI and FOR/BUD TBH were not statistically significant.
Pharmacokinetics: Following inhalation of the formoterol, glycopyrronium and budesonide combination, the pharmacokinetics of each component was similar to those observed when each active substance was administered separately.
Effect of a spacer: The use of this medicinal product with the Aerochamber Plus Flow-Vu spacer in healthy volunteers increased the total systemic exposure (as measured by AUC0-t) to budesonide and glycopyrronium by 33% and 55%, respectively, while exposure to formoterol was unchanged. In patients with good inhalation technique, systemic exposure was not increased with the use of a spacer.
Absorption: Budesonide: Following inhaled administration of this medicinal product in subjects with COPD, budesonide Cmax occurred within 20 to 40 minutes. Steady state is achieved after approximately 1 day of repeated dosing of this medicinal product and the extent of exposure is approximately 1.3 times higher than after the first dose.
Glycopyrronium: Following inhaled administration of this medicinal product in subjects with COPD, glycopyrronium Cmax occurred at 6 minutes. Steady state is achieved after approximately 3 days of repeated dosing of this medicinal product and the extent of exposure is approximately 1.8 times higher than after the first dose.
Formoterol: Following inhaled administration of this medicinal product in subjects with COPD, formoterol Cmax occurred within 40 to 60 minutes. Steady state is achieved after approximately 2 days of repeated dosing with this medicinal product and the extent of exposure is approximately 1.4 times higher than after the first dose.
Distribution: Budesonide: The estimated budesonide apparent volume of distribution at steady-state is 1200 L, via population pharmacokinetic analysis. Plasma protein binding is approximately 90% for budesonide.
Glycopyrronium: The estimated glycopyrronium apparent volume of distribution at steady-state is 5500 L, via population pharmacokinetic analysis. Over the concentration range of 2-500 nmol/L, plasma protein binding of glycopyrronium ranged from 43% to 54%.
Formoterol: The estimated formoterol apparent volume of distribution at steady-state is 2400 L, via population pharmacokinetic analysis. Over the concentration range of 10-500 nmol/L, plasma protein binding of formoterol ranged from 46% to 58%.
Biotransformation: Budesonide: Budesonide undergoes an extensive degree (approximately 90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6β-hydroxy-budesonide and 16α-hydroxy-prednisolone, is less than 1% of that of budesonide.
Glycopyrronium: Based on literature and an in vitro human hepatocyte study, metabolism plays a minor role in the overall elimination of glycopyrronium. CYP2D6 was found to be the predominant enzyme involved in the metabolism of glycopyrronium.
Formoterol: The primary metabolism of formoterol is by direct glucuronidation and by O-demethylation followed by conjugation to inactive metabolites. Secondary metabolic pathways include deformylation and sulfate conjugation. CYP2D6 and CYP2C have been identified as being primarily responsible for O-demethylation.
Elimination: Budesonide: Budesonide is eliminated via metabolism mainly catalysed by the enzyme CYP3A4. The metabolites of budesonide are excreted in urine as such or in conjugated form. Only negligible amounts of unchanged budesonide have been detected in the urine. The effective terminal elimination half-life of budesonide derived via population pharmacokinetic analysis was 5 hours.
Glycopyrronium: After IV administration of a 0.2 mg dose of radiolabelled glycopyrronium, 85% of the dose was recovered in urine 48 hours post-dose and some of radioactivity was also recovered in bile. The effective terminal elimination half-life of glycopyrronium derived via population pharmacokinetic analysis was 15 hours.
Formoterol: The excretion of formoterol was studied in six healthy subjects following simultaneous administration of radiolabelled formoterol via the oral and IV routes. In that study, 62% of the drug-related radioactivity was excreted in the urine while 24% was eliminated in the faeces. The effective terminal elimination half-life of formoterol derived via population pharmacokinetic analysis was 10 hours.
Special populations: Age, gender, race/ethnicity and weight: Dose adjustments are not necessary based on the effect of age, gender or weight on the pharmacokinetic parameters of budesonide, glycopyrronium and formoterol. There were no major differences in total systemic exposure (AUC) for all compounds between healthy Japanese, Chinese and Western subjects. Insufficient pharmacokinetic data is available for other ethnicities or races.
Hepatic impairment: No pharmacokinetic studies have been performed with this medicinal product in patients with hepatic impairment. However, because both budesonide and formoterol are primarily eliminated via hepatic metabolism, an increased exposure can be expected in patients with severe liver impairment. Glycopyrronium is primarily cleared from the systemic circulation by renal excretion and hepatic impairment would therefore not be expected to affect systemic exposure.
Renal impairment: Studies evaluating the effect of renal impairment on the pharmacokinetics of budesonide, glycopyrronium and formoterol were not conducted.
The effect of renal impairment on the exposure to budesonide, glycopyrronium and formoterol for up to 24 weeks was evaluated in a population pharmacokinetic analysis. Estimated glomerular filtration rate (eGFR) varied from 31-192 mL/min representing a range of moderate to no renal impairment. Simulation of the systemic exposure (AUC0-12) in subjects with COPD with moderate renal impairment (eGFR of 45 mL/min) indicates an approximate 68% increase for glycopyrronium compared to subjects with COPD with normal renal function (eGFR of >90 mL/min). Renal function was found not to affect exposure to budesonide or formoterol. Subjects with COPD with both low body weight and moderate-severe impaired renal function may have an approximate doubling of systemic exposure to glycopyrronium.
Toxicology: Preclinical safety data: Non-clinical data reveal no specific hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and carcinogenic potential.
No studies have been conducted with the combination of budesonide, glycopyrronium and formoterol in respect of genotoxicity, carcinogenic potential and toxicity to reproduction and development.
In animal reproduction studies, glucocorticosteroids such as budesonide have been shown to induce malformations (cleft palate, skeletal malformations). However, these animal experimental results are not relevant in humans at the recommended doses (see Use in Pregnancy & Lactation). Budesonide demonstrated no tumourigenic potential in mice. In rats, an increased incidence of hepatocellular tumours was observed, considered to be a class effect in rats from long-term exposure to corticosteroids.
Animal reproduction studies with formoterol have shown a slightly reduced fertility in male rats at high systemic exposure and implantation losses, as well as decreased early postnatal survival and birth weight at considerably higher systemic exposures than those reached during clinical use. A slight increase in the incidence of uterine leiomyomas has been observed in rats and mice treated with formoterol; an effect which is considered to be a class effect in rodents after long-term exposure to high doses of β2-adrenoreceptor agonists.
Animal reproduction studies with glycopyrronium have shown reduced rat and rabbit foetal weights, and low body weight gain of rat offspring before weaning at considerably higher systemic exposure than those reached during clinical use. No evidence of carcinogenicity was seen in rats and mice.