


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Enfortumab vedotin is an antibody drug conjugate (ADC) targeting Nectin-4, an adhesion protein located on the surface of the urothelial cancer cells. It is comprised of a fully human IgG1-kappa antibody conjugated to the microtubule-disrupting agent MMAE via a protease-cleavable maleimidocaproyl valine-citrulline linker. Nonclinical data suggest that the anticancer activity of enfortumab vedotin is due to the binding of the ADC to Nectin-4-expressing cells, followed by internalisation of the ADC-Nectin-4 complex, and the release of MMAE via proteolytic cleavage. Release of MMAE disrupts the microtubule network within the cell, subsequently inducing cell cycle arrest and apoptotic cell death. MMAE released from enfortumab vedotin targeted cells can diffuse into nearby Nectin-4 low-expressing cells resulting in cytotoxic cell death.
Cardiac electrophysiology: At the recommended dose of 1.25 mg/kg, enfortumab vedotin did not prolong the mean QTc interval to any clinically relevant extent based on ECG data from a study in patients with advanced urothelial cancer.
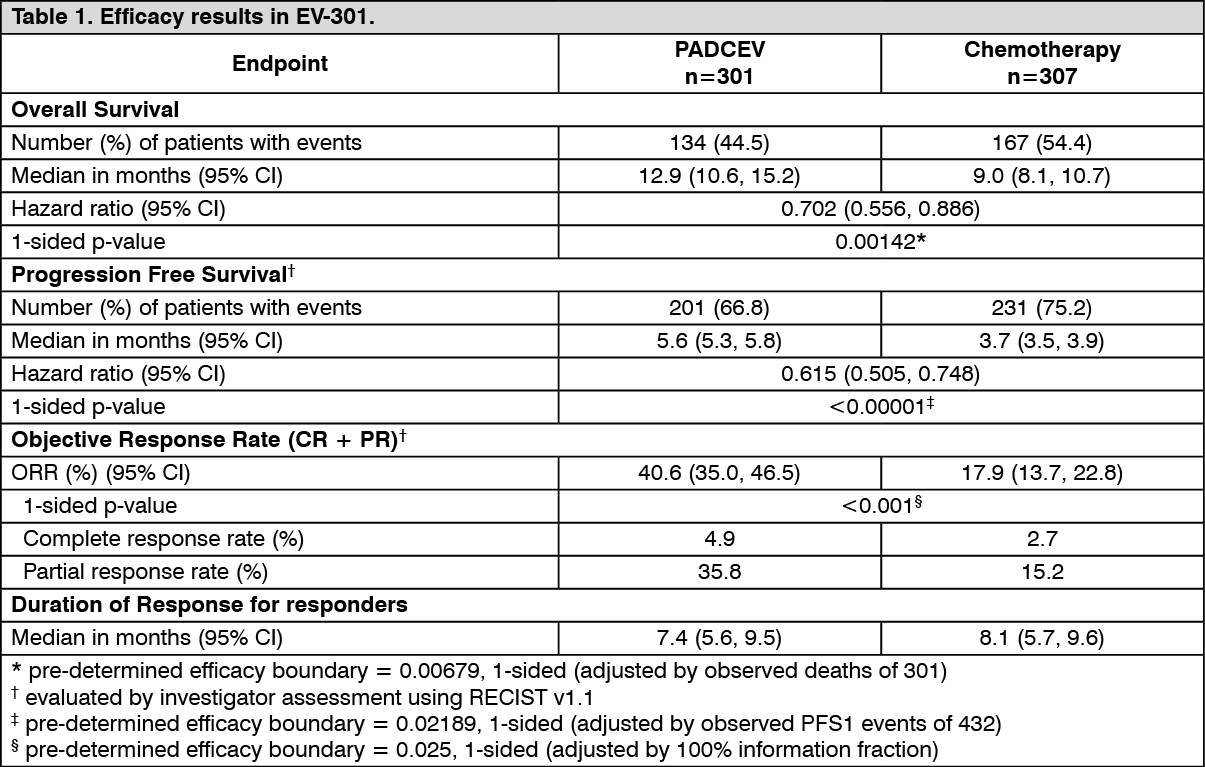
Clinical efficacy and safety: Metastatic urothelial cancer: EV-301: The efficacy of PADCEV was evaluated in study EV-301, an open-label, randomised, phase 3, multicentre study that enrolled 608 patients with locally advanced or metastatic urothelial cancer who have previously received a platinum-containing chemotherapy and a programmed death receptor 1 (PD-1) or programmed death ligand 1 (PD-L1) inhibitor. The primary endpoint of the study was Overall Survival (OS) and secondary endpoints included Progression Free Survival (PFS) and Objective Response Rate (ORR) [PFS and ORR were evaluated by investigator assessment using RECIST v1.1]. Patients were randomised 1:1 to receive either enfortumab vedotin 1.25 mg/kg on Days 1, 8 and 15 of a 28-day cycle, or one of the following chemotherapies as decided by the investigator: docetaxel 75 mg/m2 (38%), paclitaxel 175 mg/m2 (36%) or vinflunine 320 mg/m2 (25%) on Day 1 of a 21-day cycle.
Patients were excluded from the study if they had active CNS metastases, ongoing sensory or motor neuropathy ≥ Grade 2, known history of human immunodeficiency virus (HIV) infection (HIV 1 or 2), active Hepatitis B or C, or uncontrolled diabetes defined as HbA1c ≥8% or HbA1c ≥7% with associated diabetes symptoms.
The median age was 68 years (range: 30 to 88 years), 77% were male, and most patients were White (52%) or Asian (33%). All patients had a baseline Eastern Cooperative Oncology Group performance status of 0 (40%) or 1 (60%). Ninety-five percent (95%) of patients had metastatic disease and 5% had locally advanced disease. Eighty percent of patients had visceral metastases including 31% with liver metastases. Seventy-six percent of patients had urothelial carcinoma/transitional cell carcinoma (TCC) histology, 14% had urothelial carcinoma mixed and approximately 10% had other histologic variants. A total of 76 (13%) patients had received ≥3 lines of prior systemic therapy. Fifty-two percent (314) of patients had received prior PD-1 inhibitor, 47% (284) had received prior PD-L1 inhibitor, and an additional 1% (9) patients had received both PD-1 and PD-L1 inhibitors. Only 18% (111) of patients had a response to prior therapy with a PD-1 or PD-L1 inhibitor. Sixty-three percent (383) of patients had received prior cisplatin-based regimens, 26% (159) had received prior carboplatin-based regimens, and an additional 11% (65) had received both cisplatin- and carboplatin-based regimens.
Table 1 summarizes the efficacy results for the EV-301 study, after a median follow-up time of 11.1 months (95% CI: 10.6 to 11.6). (See Table 1 and figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePaediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with enfortumab vedotin in all subsets of the paediatric population in urothelial cancer (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: Distribution: The mean estimate of steady-state volume of distribution of ADC was 12.8 L following 1.25 mg/kg of enfortumab vedotin. In vitro, the binding of MMAE to human plasma proteins ranged from 68% to 82%. MMAE is not likely to displace or to be displaced by highly protein-bound medicinal products. In vitro studies indicate that MMAE is a substrate of P-glycoprotein.
Biotransformation: A small fraction of MMAE released from enfortumab vedotin is metabolised. In vitro data indicate that the metabolism of MMAE occurs primarily via oxidation by CYP3A4.
Elimination: The mean clearance of ADC and unconjugated MMAE in patients was 0.11 L/h and 2.11 L/h, respectively. ADC elimination exhibited a multi-exponential decline with a half-life of 3.6 days. Elimination of MMAE appeared to be limited by its rate of release from enfortumab vedotin. MMAE elimination exhibited a multi-exponential decline with a half-life of 2.6 days.
Excretion: The excretion of MMAE occurs mainly in faeces with a smaller proportion in urine. After a single dose of another ADC that contained MMAE, approximately 24% of the total MMAE administered was recovered in faeces and urine as unchanged MMAE over a 1-week period. The majority of recovered MMAE was excreted in faeces (72%). A similar excretion profile is expected for MMAE after enfortumab vedotin administration.
Special populations: Elderly: Population pharmacokinetic analysis indicates that age [range: 24 to 90 years; 60% (450/748) >65 years, 19% (143/748) >75 years] does not have a clinically meaningful effect on the pharmacokinetics of enfortumab vedotin.
Race and gender: Based on population pharmacokinetic analysis, race [69% (519/748) White, 21% (158/748) Asian, 1% (10/748) Black and 8% (61/748) others or unknown] and gender [73% (544/748) male] do not have a clinically meaningful effect on the pharmacokinetics of enfortumab vedotin.
Renal impairment: The pharmacokinetics of ADC and unconjugated MMAE were evaluated after the administration of 1.25 mg/kg of enfortumab vedotin to patients with mild (CrCL >60-90 mL/min; n=272), moderate (CrCL 30-60 mL/min; n=315) and severe (CrCL 15-<30 mL/min; n=25) renal impairment. No significant differences in AUC exposure of ADC or unconjugated MMAE were observed in patients with mild, moderate or severe renal impairment compared to patients with normal renal function. Enfortumab vedotin has not been evaluated in patients with end stage renal disease (CrCL <15 mL/min).
Hepatic impairment: Based on population pharmacokinetics analysis using data from clinical studies in patients with metastatic UC, there was no significant differences in ADC exposure and a 37% increase in unconjugated MMAE AUC were observed in patients with mild hepatic impairment (total bilirubin of 1 to 1.5 × ULN and AST any, or total bilirubin ≤ ULN and AST > ULN, n=65) compared to patients with normal hepatic function. Enfortumab vedotin has only been studied in a limited number of patients with moderate hepatic impairment (n=3) and has not been evaluated in patients with severe hepatic impairment. The effect of moderate or severe hepatic impairment (total bilirubin >1.5 × ULN and AST any) or liver transplantation on the pharmacokinetics of ADC or unconjugated MMAE is unknown.
Physiologically-based pharmacokinetic modeling predictions: Concomitant use of enfortumab vedotin with ketoconazole (a combined P-gp and strong CYP3A inhibitor) is predicted to increase unconjugated MMAE Cmax and AUC exposure to a minor extent, with no change in ADC exposure.
Concomitant use of enfortumab vedotin with rifampin (a combined P-gp and strong CYP3A inducer) is predicted to decrease unconjugated MMAE Cmax and AUC exposure with moderate effect, with no change in ADC exposure. The full impact of rifampin on the Cmax of MMAE may be underestimated in the PBPK model.
Concomitant use of enfortumab vedotin is predicted not to affect exposure to midazolam (a sensitive CYP3A substrate). In vitro studies using human liver microsomes indicate that MMAE inhibits CYP3A4/5 but not other CYP450 isoforms. MMAE did not induce major CYP450 enzymes in human hepatocytes.
In vitro studies: In vitro studies indicate that MMAE is a substrate and not an inhibitor of the efflux transporter P-glycoprotein (P-gp). In vitro studies determined that MMAE was not a substrate of breast cancer resistance protein (BCRP), multidrug resistance-associated protein 2 (MRP2), organic anion transporting polypeptide 1B1 or 1B3 (OATP1B1 or OATP1B3), organic cation transporter 2 (OCT2), or organic anion transporter 1 or 3 (OAT1 or OAT3). MMAE was not an inhibitor of the bile salt export pump (BSEP), P-gp, BCRP, MRP2, OCT1, OCT2, OAT1, OAT3, OATP1B1, or OATP1B3 at clinically relevant concentrations.
Toxicology: Preclinical safety data: Genotoxicity studies showed that MMAE had no discernible genotoxic potential in a reverse mutation test in bacteria (Ames test) or in a L5178Y TK+/- mouse lymphoma mutation assay. MMAE did induce chromosomal aberrations in the micronucleus test in rats which is consistent with the pharmacological action of microtubule-disrupting agents.
Skin lesions were noted in repeat dose studies in rats (4- and 13-weeks) and in monkeys (4-weeks). The skin changes were fully reversible by the end of a 6-week recovery period.
Hyperglycaemia reported in the clinical studies was absent in both the rat and monkey toxicity studies and there were no histopathological findings in the pancreas of either species.
Foetal toxicity (reduced litter size or complete litter loss) was observed and decrease in the litter size was reflected in an increase in early resorptions. Mean foetal body weight in the surviving foetuses at the 2 mg/kg dose level were reduced compared with control.
Enfortumab vedotin associated foetal skeletal variations were considered developmental delays. A dose of 2 mg/kg (approximately similar to the exposure at the recommended human dose) resulted in maternal toxicity, embryo-foetal lethality and structural malformations that included gastroschisis, malrotated hindlimb, absent forepaw, malpositioned internal organs and fused cervical arch. Additionally, skeletal anomalies (asymmetric, fused, incompletely ossified, and misshapen sternebrae, misshapen cervical arch, and unilateral ossification of the thoracic centra) and decreased foetal weight were observed.
Testicular toxicity observed, only in rats, was partially reversed by the end of a 24-week recovery period.